
“There’s something wrong with her head.”
Megan Kane was not prepared for those words from her husband, Mark. Looking closer at their newborn, Imogene, the North Liberty, Iowa, couple noticed that the right side of her forehead didn’t appear to be as full as the left.
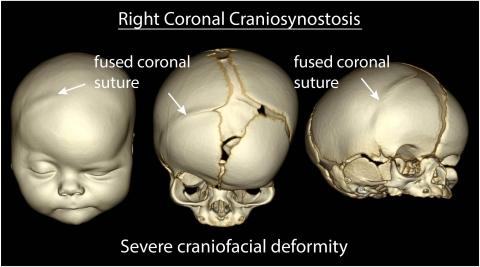
Two weeks later, Imogene’s pediatrician ordered an X-ray that confirmed their fear: Their baby girl had a fusion of the right coronal suture—two plates in her skull had fused together prematurely and would need to be separated.
Imogene, the Kanes' second child, had been born with craniosynostosis, a condition that traditionally would have meant hours of surgery. But because Imogene was diagnosed early after birth and seen quickly at the University of Iowa Stead Family Children’s Hospital, Brian Dlouhy, MD (13R, 14F), pediatric neurosurgeon, and Deborah Kacmarynski, MD, pediatric otolaryngologist, were able to employ a relatively new, minimally invasive procedure that significantly reduces the length of surgery and minimizes blood loss.
New option results in shorter surgery time



Parents play an important role in recovery

Pediatric Neurosurgery
University of Iowa Stead Family Children’s Hospital is home to one of the most experienced and comprehensive pediatric neurosurgery programs in the nation and the only nationally ranked program in Iowa.