
Iowa's most comprehensive valve disease care
A one-stop shop
For patients with valve disease or structural heart problems, the UI Heart and Vascular Center offers the most complete set of treatment options, which include catheter-based valve replacements and repairs.

First-in-Iowa procedure offers new option for high-risk patients
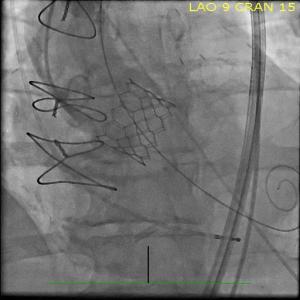
When Alan Leff appeared to have run out of treatment options for severe aortic stenosis, the UI Heart and Vascular Center found a new one for him: a highly specialized procedure called transcaval TAVR that had never been performed in Iowa before.

Horwitz and the team used the technique—a technique to bypass the patient’s diseased leg arteries—to replace Leff’s aortic valve.
Before the Aug. 11 procedure, even a short walk left Alan out of breath and weak. Without treatment, the failing valve would have greatly increased his chances of heart failure.
Leff, 84, of University Heights, Iowa, had been diagnosed with mild stenosis about two years earlier, but an exam in May found that the condition had advanced significantly. The valve needed to be replaced soon, but open-heart surgery was too risky.
Because Leff has peripheral artery disease, he wasn’t a good candidate for a standard TAVR procedure. A CT scan showed that none of his arteries would allow reasonable access to the heart using a catheter.
Horwitz recognized that transcaval TAVR offered Leff the option he needed to have the valve replaced. In transcaval TAVR, the catheter is advanced through veins instead of arteries. When it reaches a vein that is parallel to the aorta, the catheter crosses into the aorta, and the artificial valve is placed just like it would be during a standard TAVR procedure. At the end of the procedure, the hole in the aorta is closed with a specialized plug.
Leff had the procedure on a Tuesday and was home by the following Sunday. His walks are no longer hampered by his failing aortic valve, and within weeks he was making noticeable progress.
“I’m to the point where I can walk a block without having to stop,” he says.
But what impressed him the most is how the UI Heart and Vascular Center worked to give him the care he needed.
“Dr. Horwitz could have simply said I wasn’t a candidate for TAVR,” he says. “But he didn’t. He reached out and sought something else for me. It was very gratifying to be working with them. It was a confidence-builder.”
The addition of transcaval TAVR means UI cardiologists have the most complete set of treatment options for severe aortic stenosis, including options for patients with the most complex cases.
A shifting field for surgeons
Just as catheter-based procedures were taking off, cardiac surgeons, like Bashir, started considering how to make traditional surgeries more efficient.
“I was lucky to be able to train in that era when I could see that this field was going to have a lot of changes. I needed to be able to embrace that and take it to the next step,” he says.
That next step was the UI Minimally Invasive Cardiac Surgery Program, started by Bashir in 2018.

With robot assistance and tiny cameras, a cardiac surgeon accesses the heart through small incisions on the left side of the chest to perform bypass surgery, and the right side of the chest to perform valve replacements and most other heart procedures.
“We’re applying the gold standard therapy, open-heart surgery, but we’re doing it in a less-invasive way,” Bashir says. “We have many patients who are extremely happy now because they were going from one center to another as they simply didn’t like the idea of going through open-heart surgery. They come here because they hear about this approach.”
These patients typically leave the hospital after three days and recover in two to four weeks, according to Bashir, whose practice has shifted significantly toward this new approach. Roughly half to 60% of his cases are completed in a minimally invasive way.
“If it was up to me, I’d do everything less invasively, but some patients bring a lot of medical challenges with them, so it’s not as practical to do it that way for everyone,” he says.
Patient selection is key in all levels of care. For example, younger patients without other complex health issues may experience a greater benefit, over the long term, from open-heart surgery. And now the minimally invasive approach gives them a faster recovery option. Minimally invasive surgeries are also beneficial for older patients allowing them to avoid a large sternal incision.
“This is a niche program in Iowa in that we are the only center that does this in a really efficient manner with a higher volume of patients with complex cases,” Bashir says.
Tony Craine was a contributing writer.
Minimally Invasive Heart Surgery
University of Iowa Heart and Vascular Center surgeons offer minimally invasive heart and thoracic surgery with the state's largest and most experienced physician team in these state-of-the-art procedures.